
Rotator Cup, Rotor Cuff, Rotary Cuff – we’ve heard it called many things – but just what is your ‘Rotator Cuff’?
Many people with shoulder pain present to a physiotherapist, or doctor, and get diagnosed with a rotator cuff injury. These people can be left confused, because they don’t fully understand what exactly that is, or why it matters. All they know, is their shoulder hurts, and they want it to stop.
The first step to rehab is understanding your injury, and understanding why or how you hurt.
What is a Rotator Cuff?
Is it a muscle? A ligament? A tendon? A bone?
The rotator cuff is a couple of those things. It is a collection of muscles. Four muscles to be exact. Muscles turn into tendons, and tendons attach muscles to bones. Therefore, muscles allow us to move our bones.
The short answer: the rotator cuff is 4 muscles and their associated tendons.
Here’s a picture:
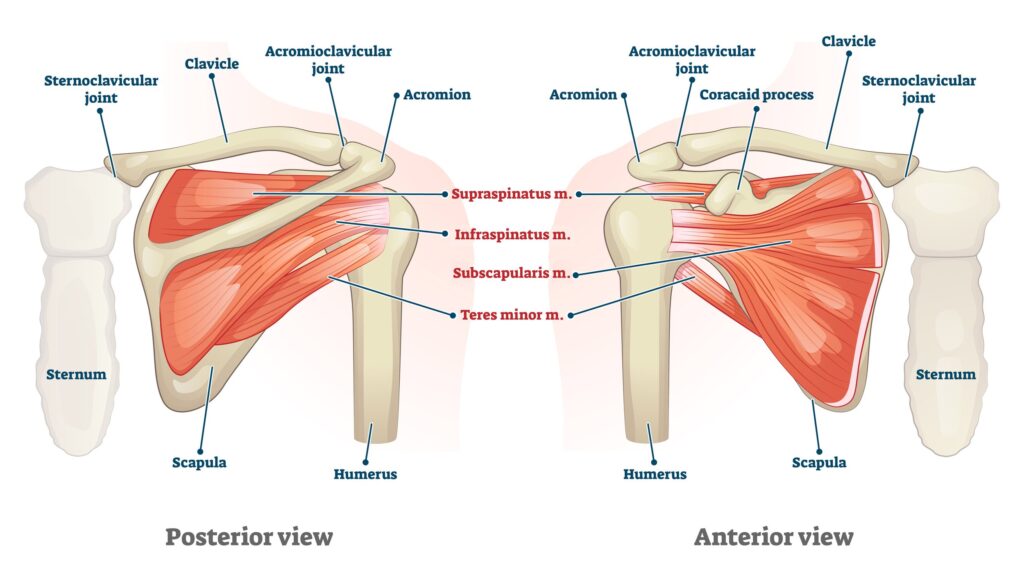
In the picture, the red parts are the muscle bellies, the white parts are the tendons. These 4 muscles start on your shoulder blade (scapula) and attach to your upper arm (humerus). The left part of the picture shows what it would look like from the front (looking through and past your torso/rib cage). On this side of the shoulder blade, we have 1 of the 4 rotator cuff muscles: the subscapularis muscle. The right part of the picture shows what it would look like from the back, with the supraspinatus muscle on the top, and two muscles, the infraspinatus and teres minor, coming from the big body of the shoulder blade.
Individually (and simplified), these muscles do the following movements:
- Supraspinatus: arm abduction (lifting your arm up to the side)
- Infraspinatus and Teres Minor: external rotation (turning your arm outwards)
- Subscapularis: internal rotation (turning your arm inwards)
However, like most things in our body, it’s not that simple. The rotator cuffs’ main job is to keep the humeral head (ball on the end of your upper arm), centred in the glenoid cavity (the shoulder socket) (see below).
As you can see, the glenoid cavity (shoulder socket) is pretty shallow, so the rotator cuff works quite hard in certain positions – for example, when working overhead or when reaching. (The cavity is this shallow to allow our shoulders to be super mobile – and don’t worry, there are other things that help – but that’s a different blog post!).
How do you hurt your rotator cuff?
You can injure your rotator cuff in many ways, but here are some of the more common ways:
- Repetitive use (using your shoulder a lot tires out the rotator cuff and it gets painful)
- Overreaching (or lots of reaching)
- Overhead work (working with your arms above your head, especially for a long time)
- Trauma or falling (like a body-check in hockey, or falling on your arm)
- Combining these things – like repetitive overhead reaching, can be very strenuous on your rotator cuff
A Word on Injury ‘Names’
When you injure a muscle, it’s called a strain (you sprain a ligament). So therefore, a muscle injury to 1 (or more) of your 4 rotator cuff muscles is called a rotator cuff strain. If a strain worsens, or it is a big strain, it can become a partial tear, and progress further to a full tear. A complete tear is when the muscle detaches from the bone.
Note: These things can sound scary, but not all of these require surgery, and it is important to get a proper assessment to determine the appropriate plan of action!
The above names are sometimes used for rotator cuff injuries, but more commonly, people will be told they have rotator cuff tendinitis.
But what is that? It simply means that the tendon(s) of the rotator cuff are inflamed (the ending ‘-itis’ means ‘inflammation’). Remember, the tendon is what attaches the rotator cuff muscle to the bone (see above pictures).
How do I know if I even need rotator cuff surgery?
Typically, to qualify for a surgical rotator cuff repair, the following statements are true:
- You have significant shoulder pain that is greatly limiting your ability to complete your activities of daily living (i.e. get dressed, sleep, work)
- You have imaging results (i.e. an MRI) that show rotator cuff damage (and this damage is ‘fixable’ with surgery)
- You have tried to reduce your pain and improve your function through virtually every other conservative option, including a significant bout of physical therapy
- Conservative options include, but are not limited to: physiotherapy, massage therapy, chiropractic care, acupuncture, and injections
Do I have to do pre-operative physiotherapy?
In short, yes, you should. It helps in the following ways:
- Helps you understand what to expect with surgery and postoperatively (just like this blog post should!)
- Helps strengthen muscles to their maximum potential (not just rotator cuff muscles, but also neck, back, and other arm/shoulder muscles)
- Improves your range of motion to help limit stiffness in all associated joints
- In some cases, physiotherapy eliminates the need for surgery in the first place!
What else should I do before rotator cuff surgery?
- Understand what you’re getting yourself into (read on!)
- QUIT smoking (smoking can increase rotator cuff retear rates by up to 25%!)
- Eat well, and take steps to improve your overall health
- Organize assistance for after surgery (you’ll have trouble bathing, dressing, and cooking with just 1 arm!)
- Assistance may be needed for a couple of months – for example, you will not be allowed to drive for at least 6 weeks post-op.
How is rotator cuff surgery performed?
Every surgeon has their individual preferences, however, most surgeons do arthroscopic rotator cuff repairs.
Arthroscopic means that the surgeon will use a tiny camera called an arthroscope. The arthroscope is inserted into your shoulder via a fairly small incision.
The tools required to fix your rotator cuff are inserted through additional small incisions.
Therefore, you’ll likely only have a few small incisions around your shoulder!
To repair the rotator cuff muscle/tendons, the surgeon will use ‘sutures’ and ‘suture anchors’ (or ‘anchors’ for short).
The sutures and anchors will help to hold tears together or help to attach a torn tendon securely to the bone.
These sutures and anchors are not removed. They are safe to stay in your shoulder for life.
Disclaimer:
Before we get into the next part of this blog post, it is important to note that everything in this blog post is for information purposes only.
This blog post is not intended to be strict medical advice. As previously mentioned, everyone is an individual, and therefore, individual variances do occur.
It is important to consult your physiotherapist, surgeon, and/or doctor for the most applicable advice for you.