Pain pain go away, come again another day leave right now and stay away.
Have you ever experienced physical pain?
I’m willing to bet you have. What happened to cause your pain? Did you fall down the stairs? Did you get tackled playing rugby? Were you in a car accident? Did you just wake up with pain not knowing what you did? Does any of this really matter?
What is Pain Science?
Pain is complicated. Much like my relationship with donuts.
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.
That’s a lot of words.
Simply put, pain is “an unpleasant experience or feeling sent out by the brain in response to perceived threat”. This is based on many different factors, which we will try to clarify throughout this blog post. Here’s the first couple things to consider:
- Pain is an experience – ‘experiences’ are individualized, based on many different factors. They are unique to the individual and forever changing.
- Pain is an output from the brain – in every instance, no matter what, the brain sends pain to the affected body part.
- Pain is sent in response to perceived threat – this threat can be perceived due to a very real threat (like a broken bone), or from a pending threat to our well being (like the pain we feel when carrying a hot bowl from the microwave to the table (the threat of a burn is pending)).
- The perceived threat does not apply solely to our physical wellbeing, but to our wellbeing in general – we may also feel pain when our emotional, psychological, or social wellbeing is threatened (think of the chest pain you feel when your feelings are hurt).
- Humans are bio-psycho-social beings – meaning our make-up and function relies on biological (physical) systems, psychological (thought-related) systems, and sociological (environment-related) systems – more on this throughout the blog!
Some of this may be difficult to conceptualize, because, as I was, you were likely raised with the understanding that ‘pain = damage’, and therefore ‘more pain = more damage’. The reason I was raised that way is because for a long time, we thought that was true. Then researchers decided to test these theories, and the results were quite surprising.
Have you ever experienced pain that worsens with expectations, stress, or anxiety?
Many people “carry stress in their shoulders/neck”, and have experienced neck and shoulder pain/tightness/soreness when stress levels are high at work or at home. This is often the most relatable scenario to help people understand pain(s) that can come from non-physical damage. To keep things simple, pain can arise from any scenario in which our brain believes our well-being is being threatened, including:
- High levels of stress
- High levels of anxious thoughts or depressive feelings
- Poor sleep hygiene
- Fear avoidance (avoiding things in fear that it will hurt)
- The expectation of pain
- Beliefs and meanings about pain – i.e. pain will worsen if ‘x,y, or z’ happens
- Nociception (this is the science word for the chemical/thermal/mechanical sensations that travel to the brain when harmful/potentially harmful stimuli are sensed).
- A combination, to any degree, of some, or all of the above.
- As mentioned, pain is complicated.
Because pain is a perception, anything that alters this perception can alter pain. Let’s look at some cool science.
Cool Pain Science!
Consider two people, each sitting alone in a room with a button in front of them.
When they press the button, they will be shocked. One of the two people is in the “powerful shock” group, while the other is in the “minimal shock” group.
Each person has been told what group they are in – that is, person 1 has been told that when they press the button they will receive a powerful shock, while person 2 has been told that when they press the button the will receive a very minimal shock.
Then, researchers shock both participants with the exact same shock.
Which of the 2 people reports more pain? That’s right, the person who expected it to be higher. They had been led to perceive that the shock would be quite intense, and thus, they report it so. While person 2, who expected a minimal shock, reports minimal associated pain.
This is an excellent example of how expectations can alter the reported feelings of pain. What’s more interesting is that the researchers also measured the biological (brain chemical) markers of pain, and they also changed based on expectations.
You can read more about this phenomenon here if you like.
This phenomenon is related to something called the “nocebo-effect”.
Most people have heard of a “placebo”, and the “placebo-effect”. In short, the placebo-effect is when there is an improvement in the condition of a patient that occurs in response to treatment but cannot be considered due to the specific treatment used. Or, due to the expectation that they will improve, they do, in fact, improve.
The “nocebo-effect” is essentially the opposite. If the client has the expectation that they will worsen, they will, in fact, worsen.
Have you ever been told “you should never [insert activity here] again”?
Consider this statement: “because of your knee injury, you should never run again”.
In a very select few cases, this may be true, but it’s often an poorly-assessed over-exaggeration.
In many cases, statements like these can create predetermined expectations of pain, especially when they come from the mouth of a healthcare provider.
Knowing that you should “never run again” encourages the brain to feel as though the knee is significantly damaged, vulnerable, or ‘broken’.
However, the human body is:
- Extremely individual
- Highly adaptable
- Very resilient
Thinking about this example: “you should never run again” – which is blunt, and apparently all-encompassing, consider these statements instead:
- What does ‘running’ mean to you?
- Do you want to jog across the street in a hurry? Or sprint as fast as you can?
- Do you want to run 5km for health, or a marathon 5x/year?
- Do you want to run around playing with your kids in the backyard?
- What is your goal with running?
When told that “you should never run again”, it’s possible that each time some version of ‘running’ happens, the expectation of pain/dysfunction will be intensified, and the feeling of ‘being broken’ will rear its ugly head.
This may lead to increased medication intake, and increased health-provider (i.e. physiotherapist) costs.
However, when considering some of those other questions, it’s often possible to work with a trusted health care provider to reach a reasonable goal given patient, consistent, and appropriate progressions to running (for example).
Have you ever experienced pain despite not remembering what you did to hurt yourself?
If your pain came on and you can’t seem to pinpoint what started it all, please keep in mind the other aspects of your pain, as in many cases, they can be the primary culprit(s).
This may be a difficult concept to think about. The circumstances/environments in which we were raised lead us to believe that the pain came from the most recent event/scenario/physical threat – like “my back hurts because I slept on a bad mattress”, or “I had to sit in the car for 3 hours”.
However, in many cases in which there was no trauma or mechanism of injury (keep in mind, the human body is extremely resilient – so it’s hard to significantly injure without trauma/high loads), blaming our recent pain on a single night of sleeping on a poor mattress may be akin to blaming your $0.00 dollar bank account balance on the most recent Tim Horton’s you bought.
It’s possible a single event isn’t the major problem, more an accumulation of small things (stresses, anxieties, poor sleep, and an uncomfortable mattress) that lead to a perceived threat to your wellbeing – and therefore – the experience of pain.
Have you ever had your doctor order an x-ray or MRI, to figure out what’s causing your pain? (or thought about how this might make your pain worse?)
Another common strategy taken by medical professionals when treating people in pain is to do medical imaging – an x-ray, CT scan, ultrasound, and/or MRI.
The hope here is that the image will show a structural fault, and thus, the pain source.
If only it were that easy.
As per the theme of this blog, pain is much more complicated than having a physical “fault”, and there is now unarguable proof that imaging findings (the degree of physical fault) and the degree of pain/dysfunction are poorly correlated.
Here’s the science:
1. This study by Brinjikji et al. (2015) looked at the imaging findings of over 3000 people’s spines who have NO pain. This graph shows the rates of various structural “faults”/”damage” found on these images:
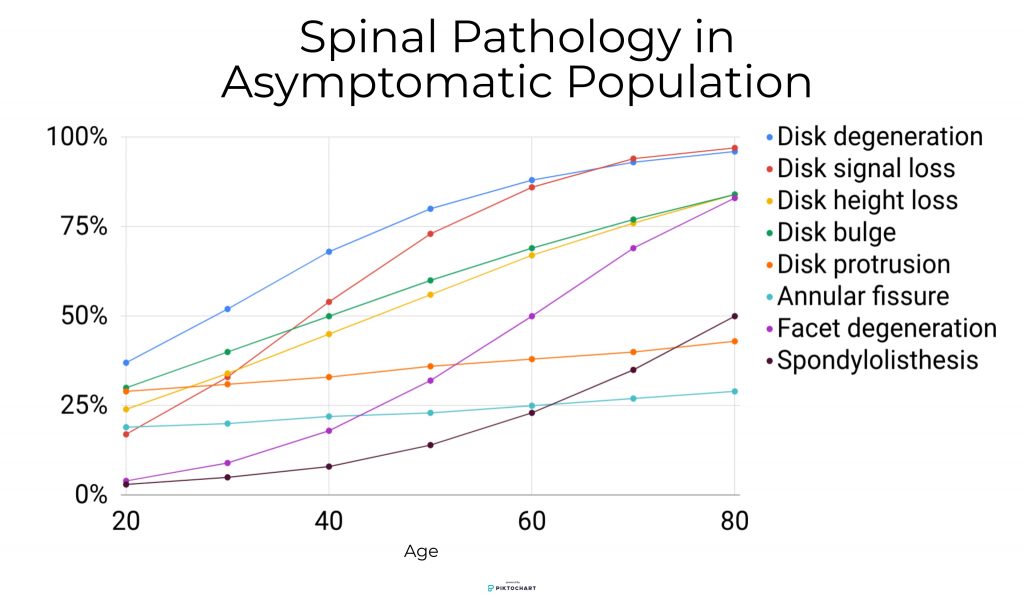
Looking at this graph, we can see that the percentage of people with these “faults” increases steadily with age (in all categories).
So what does this mean? First, it likely means that these findings are more akin to “age-related changes”, than they are to significant structural problems, especially if they are present when the person has sustained no trauma.
We’ll often encourage clients to consider these findings like wrinkles, or grey hair – just on the inside.
We all get grey hair, but the amount we get, the age at which we get it, and how we feel about it is more individualized.
Second, these findings are all people without pain, meaning even if you have these imaging findings, you can still live completely pain-free.
2. As mentioned previously, expectations can play a significant role in the amount of pain we feel.
So consider this:
You have some back pain, and you’ve had an MRI. The MRI report says you have “moderate degenerative disc disease”.
Consider first how those words make you feel – “degenerative”, and “disease” are words with negative connotations to them, and it’s quite normal to feel like you might be severely injured.
The word “degenerative” also means that things are worsening, so it’s easy to see how people can feel quite concerned when hearing about these findings.
This study by Webster et al. (2013) concludes that “the receipt of an early MRI…was associated with worse outcomes, even after controlling for severity and demographic factors”.
This means that getting an MRI may actually make you less likely to improve.
Why is this? There’s probably no single specific reason.
But we do know that the act of getting an MRI changes nothing physically about the back – only the “psycho-social” factors could change.
Perhaps the act of receiving an MRI has a ‘nocebo-effect’ to it, in that the person believes that if they need an MRI in the first place, they must be quite injured.
Or, maybe it has to do with the written report provided to the person after they receive their MRI. This report may be a page long with various medical words stating “moderate degenerative disc disease”, “disc bulging”, “stenosis of the central canal”, etc. all as findings.
To someone with little medical knowledge, reading a 3 paragraph long report outlining the findings of their image can be threatening based solely on the length of the report.
Now consider if they then google all the findings separately and come up with a laundry list of “problems”.
Yikes.
3. A final example. Here’s the short and sweet version of this study by Herzog et al. (2017):
- A single person with long standing low back pain
- Visits 10 different medical centres to have 10 different MRIs (all within a 3 week period)
- MRI results reported on by 10 different radiologists
- 49 total different “issues” were reported
- ZERO issues were reported in all 10 MRI scans
So what does this mean? It means that there is a very high variability in the findings reported within a single patient in a very short time frame.
It also means that MRIs do not tell us what is causing pain (if they did, then all reports would have been the same).
MRIs should be used when trying to exclude more serious issues (i.e. cancer, tumour, or broken bone).
So, does it matter where your pain comes, and why you feel it?
Of course it does!
Just because pain has what we call ‘psycho-social’ components (the parts of your pain experience that come from stress, anxiety, or fear), the biological components (the tissue damage from a broken bone) are also important. That said, over time, researchers have learned that although pain often begins with some level of biological deficit, it will often persist due to the psycho-social components.
It should also be noted that just because pain has “psycho-social” components, it certainly doesn’t mean that the “pain is in your head”, and it certainly doesn’t make the pain any less real.
It simply means that when humans feel pain, it’s due to a complex, multi-factorial experience, individualized to each person’s situation.
So, if an individual feels pain, it is the individual that needs treatment, not only their ailing body part.
Thus, if you were tackled in rugby and sprained your ankle, or you were injured in a car accident and strained your neck muscles – it will be important to rehabilitate the physical components of your injury.
Just remember to consider the psycho-social components of your injury, as sometimes, they require extensive treatment as well.
At Strive Physiotherapy & Performance, we are committed to providing an in-depth assessment to ensure we can work together to find the best plan of action for each individual client. Call us at 519-895-2020, or use our online booking tool on www.strivept.ca to book an appointment with one of our knowledgeable physiotherapists, and they will be sure to help you understand your individual pain.
Take care,
Tyler Allen
Physiotherapist at Strive Physiotherapy & Performance