No two people are alike. No two healing and recovery stories are the same. We usually don’t even have a good comparator for someone else in the same boat as us when we get hurt.
But I did, and I still do. I’ve been excited to write this blog for a long time, and I’m glad it’s happening.
It will outline two people who broke the same bone, the same week. The similarities certainly don’t end there, which helps a lot from a comparing “apples to apples” stand point. That being said, the healing and recovery processes also looked quite different (and still do).
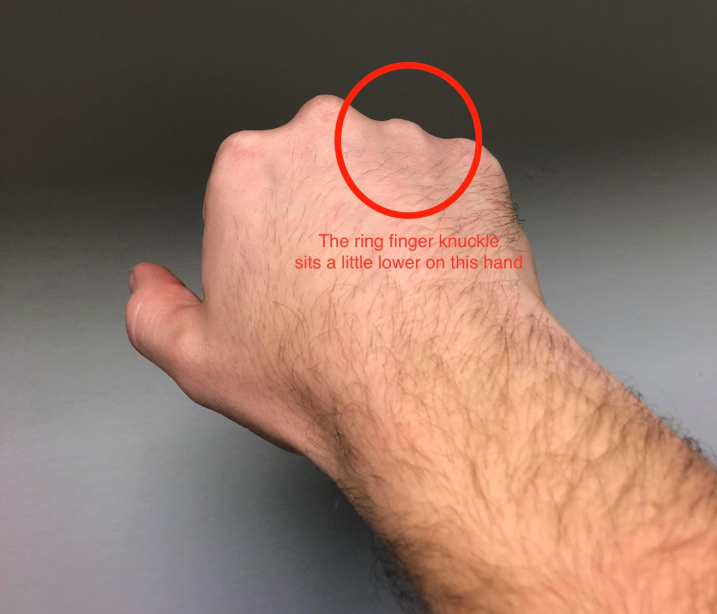
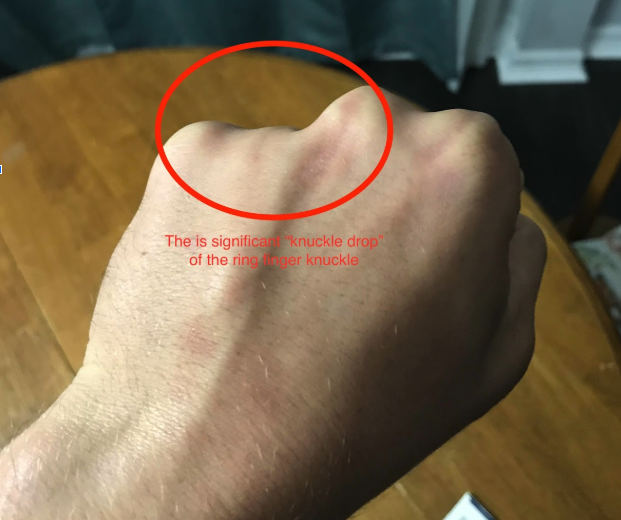
Meet our two subjects – as they are today:
| Tyler Allen (hey, that's me!) | Matt Vonk |
|---|---|
|
Demographics:
Current life:
At time of fracture:
|
Demographics:
Current life:
At time of fracture:
|


So why is it that two guys, who are of similar age, with no other medical conditions, who broke the same bone, the same week, look this different 6 years down the road? To fully understand this, we should first understand bones and how they heal.
Bone Anatomy
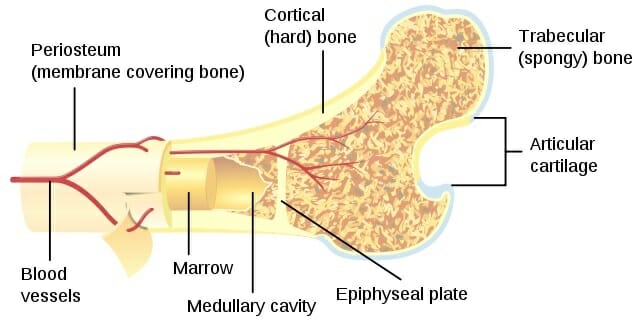
As shown in the above picture, most bones have good blood supply (see the blood vessels intertwined), so they generally heal well. For the purposes of this blog, this is probably enough information on the structure of bones.
How bones heal:
Bone healing is more of a regeneration than a repair. Essentially, the body creates new bone from within the fracture site. This picture outlines the simplified process of how that happens:

There’s a few things worth noting about bone healing.
First, is that “clinical union” (when the cast usually comes off) is when there’s a ‘bony callus formation’ (this usually takes approximately 6 weeks – but varies person to person).
Second, during the callus formation stages, bone is laid down in a woven matrix (kind of just slapped in there) – so it’s not very strong (it gets stronger during the remodeling phase). Bones will continue to heal based on their loading environment. This is called Wolff’s Law, in which “the bone of a healthy person will adapt to the loads under which it is placed.” So, if you increase the load on a particular bone, the bone will adapt to accept more of that load (it will get stronger more dense) .
The opposite is also true, if loading on a bone is significantly decreased, it will become weaker and less dense.
If you’re so inclined, here’s bone healing in a little more detail (otherwise, scroll down and skip this part):
There are four discrete stages of healing within the 2 stages:
- Hematoma formation (inflammatory) phase
- Area for new bone formation is filled with new blood
- Border tissues also often traumatized = focal necrosis and reduced blood flow
- Effective bone healing will have inflammatory stage characterized by release inflammatory molecules (which signal the bone to bring blood flow to the area), then there will be an increase in blood flow to the area (which brings in nutrients and takes away waste)
- Soft callus (fibrocartilaginous callus) formation phase
- Formation of connective tissues, including cartilage and formation of new capillaries (blood vessels) from pre-existing ones
- Body creates a cartilage matrix that is woven over the fracture site – chemicals then prepare this to be calcified (turned into new bone)
- Hard callus (bony callus) formation phase
- Body carefully removes parts of the initial matrix and tissues that formed in the site, and replaces it with stronger bone.
- Osteoblasts (bone building molecules) can form woven bone rapidly, but it is randomly arranged and thus mechanically weak
- This bone is aligned in response to loading environment
- This bridging of woven bone is constitutes “clinical union”
- Once “clinicall union” has happened, the cast usually comes off – typically takes about 6 weeks
- Remodeling phase
- The bone is remodelled to build stronger over time based on how it’s loaded
- Woven bone replaced by stronger lamellar bone by the orchestrated action of osteoclast bone resorption and osteoblast bone formation
So, I repeat: why is it that two guys, who are of similar age, with no other medical conditions, who broke the same bone, the same week, look this different 6 years down the road?
Let’s look at how the healing stages went.
| Tyler | Matt | |
|---|---|---|
|
Steps taken immediately after fracture:
|
Stopped playing soccer. Drove to hospital for an x-ray. Immobilized fracture.
|
Made hand into a fist and continued to play an entire university football scrimmage. Then mentioned it was sore, got an x-ray. Immobilized fracture.
|
|
Immobilization technique and time:
|
Custom-made removable light weight splint. Worn 24 hours a day except when washing hands. Fingers splinted at a slight angle to encourage normal tendon length.
|
Cast. Worn for up to a week at a time, then fracture re-set and cast replaced (it was soaked in sweat). Fingers casted straight each week. |
|
Total time immobilized: |
5 weeks |
10 weeks |
|
Life activities completed while hand was broken:
|
Completing Master’s Degree in Physiotherapy – classes, labs, homework
|
Completing a Master’s Degree in Kinesiology (Neuroscience) – classes, labs, research
|
|
Sport/exercise activities while hand was broken: |
Occasional run, occasional cycling. Self-limiting.
|
Continued to play in all university football games and practices. Hand casted, then wrapped in padding to try and limit further fractures.
|
Regardless of your medical expertise, it is likely that you noticed some major differences when reading the above table.
As mentioned, bones heal based on the amount of load placed on them. When I (Tyler) broke my hand, I immobilized it within a few hours and then did essentially nothing with that hand for 5 weeks – this was enough time for the bone to heal.
The amount of extra load placed on my hand was minimal, so my body built enough bone to heal my fracture, and then with rehabilitation it remodeled to a very little amount of extra bone.
Matt, however, played another hour or 2 of high level football (he’s a lineman, by the way) – pushing, blocking, grabbing, and tackling people. Then, he immobilized it. But, during this immobilization period he continued to play football multiple days per week. The load he was placing on his bone week after week was substantial. In response to this substantial load, his body kept laying down more and more bone – it felt as though he needed it.
So, in total, it took his bone twice as long to obtain “clinical union”. You might also be thinking: how is it that someone can play varsity level football with a broken hand, especially when they’re a lineman?
Here’s how:


Matt is a beast. They wrapped it up each week, and he played his heart out. You might also be thinking: “was it worth it?”. So I asked him, and this was his answer:
“It was absolutely worth it - it gave my team a chance to win. It’s nice to know I can push through that type of discomfort. The risk being I would lose some use of my hand but my doctor would X-ray and put it back into place each week. It’s perfectly functional. It’s my non-dominant hand, so it’s weaker than my right side, and the strength took awhile to come back. It just looks really different…But I played 5 years of professional football with it and never hurt it again."
Matt Vonk
There’s Matt (#53) as a member of the Saskatchewan Roughriders, the #50 for the Montréal Alouettes. He went on to play 5 years in the CFL. As he said, his hand is fine.
These cases are a good example of the “risk-reward” conversation often had in a rehabilitation setting. Matt’s risks – more hand fractures, slower healing time – did not outweigh the potential reward – becoming a professional athlete. Tyler’s risks – flunking out of physiotherapy school, not being able to become a manual therapist – far outweighed any “rewards” that could have come from not following a strict immobilization protocol.
If you remember back to the very beginning of this post, you might see that since retiring from the CFL, Matt has taken a liking to jiu jitsu. Turns out, he’s pretty good at that too:


Individuals heal in individual ways. Although the physiology of bone healing was likely quite similar for Matt and I, the environment in which our fractures healed was drastically different.
Bones heal in how they’re loaded. We use casting for broken bones to try to eliminate deformities, and to promote maximum function post-healing. As we learned, the bone will remodel for 2 years post-fracture, which says a lot about the importance of rehabilitation. Once your cast is off, having a physiotherapist teach you how to safely regain range of motion, strength, and function will help ensure your bone completely heals the best it can.
At Strive Physiotherapy & Performance, we are committed to providing an in-depth, one-on-one assessment to ensure we can work together to find the best plan of action for each individual client. Broke a bone? Call us at 519-895-2020, or use our online booking tool on www.strivept.ca to book an appointment with one of our knowledgeable physiotherapists, and they will be sure to help you understand your injury.
Take Care,
Tyler Allen
Physiotherapist at Strive Physiotherapy & Performance