This blog post was encouraged by an interesting editorial paper of the same name: Musculoskeletal Healthcare: Have we over-egged the pudding? By Maher et al. 2019 . The term “over-egging the pudding” is an analogy (used in Australia more than Canada – the authors are all Australian). The analogy applies when something is being “overdone”. For us non-culinary folk, making the “perfect” pudding involves the perfect ratio of “eggs”. Too little egg, the pudding falls apart, too much and the pudding goes rubbery.
When applying this conversation to medicine or physiotherapy, most people would understand the risks of receiving “too little” healthcare, but have we considered the consequences of receiving “too much” healthcare?
 References in the table:
1 health.gov.on.ca
2 bmj.com
3 Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ 2017;257:j1982.
4 Blogpost: Knee Scopes
References in the table:
1 health.gov.on.ca
2 bmj.com
3 Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ 2017;257:j1982.
4 Blogpost: Knee Scopes
Overdiagnosis and Overtreatment
The aforementioned editorial discusses just that; the progressively more common occurrence of “too much”. This may mean that there is an “over-diagnosis”, which, in turn, may lead to “over-treatment”. Let’s explore further. The editorial by Maher et al. (2019) describes an “overdiagnosis” as “an unwarranted diagnosis that leads to unnecessary treatments that do not benefit patients and that wastes healthcare resources that could be better used elsewhere”. Of course, there is a cost consideration with this – for example – OHIP paying for an MRI (Magnetic Resonance Imaging) that would clinically provide little benefit. But what must also be considered are the direct effects (i.e. radiation exposure), unintended effects (i.e. nocebo-related effects), or psychological consequences. This is certainly something that I personally feel strongly about. At what point is it highly necessary to assess (and therefore attempt to diagnose) via more in-depth methods, such as an MRI?Do You Need an MRI?
One of the more common questions we hear from clients is “do you think I need an MRI”, or they simply state “I think I need an MRI”. Now don’t get me wrong, in certain scenarios, MRIs can be highly beneficial, and are definitely warranted. But there are a few things to consider first.- Will the results of the MRI (or any medical image for that matter – x-ray, ultrasound) alter the treatment plan?
- Example 1: Client has insidious onset back pain after a highly stressful work trip in which they slept and ate poorly, and neglected exercise. There has been no trauma, and the client reports no concerning findings. It is HIGHLY UNLIKELY that this client would benefit from an MRI (more on that later). The results of an MRI are unlikely to change the treatment protocols – return to movement, improving sleep/diet/stress management/exercise habits.
- Example 2: Client has significant low back pain after getting hit by a car when cycling. They have significant numbness and tingling in both legs, and they are unable to pass urine, despite feeling like they have to and trying to. This person is likely to benefit from further imaging (i.e. an MRI) to help RULE OUT a significant pathology (such as a fracture, or spinal cord injury). It is possible that the results of an MRI would change treatment protocols – need for emergency surgery.
- Will the benefits outweigh the risks?
- Potential benefits/positives include: finding sinister pathology that requires treatment, eases client’s mind
- Potential risks/negatives include: cost to healthcare system, psychological impact of findings, nocebo-related effects, time to receive MRI (often weeks to months in Canada), findings unlikely to alter treatment plan
- You can have “structural changes” – which will be reported on your MRI – but they often do not correlate well with pain or dysfunction. Meaning, you can have big changes and no pain, or no changes and significant pain.
- This study by Webster et al. (2013) concludes that “the receipt of an early MRI…was associated with worse outcomes, even after controlling for severity and demographic factors”. This means that getting an MRI may actually make you less likely to improve.
- MRI findings have a very high variability (meaning different findings are reported by different radiologists, even if they read the same image)
Why Does Overtreatment happen?
It would be awesome if the answer to “why does this happen?” was an easy one. Unfortunately, it’s likely highly complex, and related to many possible drivers. There may be educational deficiencies amongst healthcare professionals (and the general public), commercial/financial incentives, reluctance to change the status quo, or cultural/personal beliefs. Education is a great place to start, hence this blog post directing you to such an insightful editorial. That said, it’s likely that we need further and more robust research to help us understand the why, how, and what we can do about it.Knee Pain and Knee Scope Overdiagnosis
I’ll borrow wording for my headings (overtesting, overdetection, over-definition, over-treatment) from the editorial to outline an example that is all too common in the physiotherapy world: knee pain and knee arthroscopy (a surgery in which small instruments are inserted into your knee joint to “clean up” the inside surfaces of your knee). Hopefully this example will help you understand the potential impact of “over-egging the pudding”, with respect to someone’s knee pain.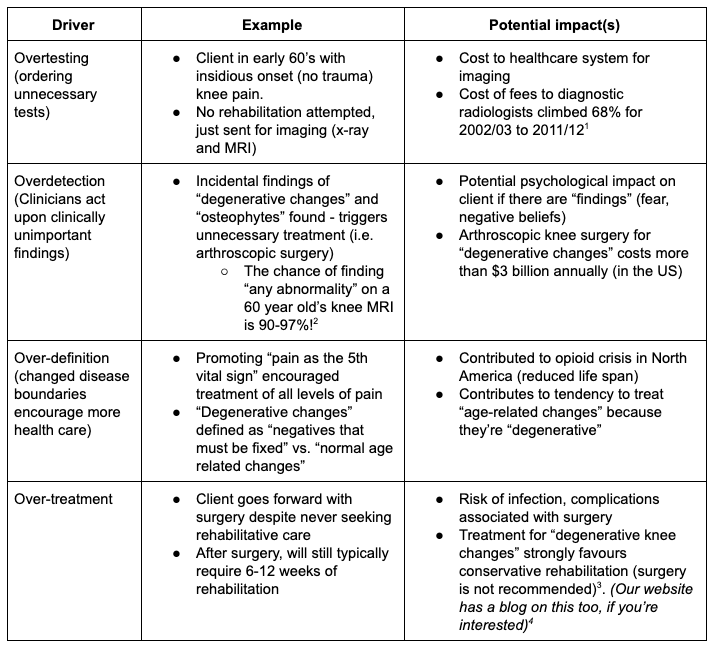 References in the table:
1 health.gov.on.ca
2 bmj.com
3 Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ 2017;257:j1982.
4 Blogpost: Knee Scopes
References in the table:
1 health.gov.on.ca
2 bmj.com
3 Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ 2017;257:j1982.
4 Blogpost: Knee Scopes
Now visualize the alternative course of action.
What could (should) have happened:- Client in early 60’s with insidious onset (no trauma) knee pain
- Gets referred to physical therapy
- Learns about: self-management principles, the complexity of pain, what’s considered “normal, age-related changes”, safe and effective exercises
- After 6-12 weeks of rehabilitation (or less!), client feels less pain and is empowered to confidently manage their own knee (remember, this 6-12 weeks of rehabilitation happens either way!)
- No radiology-related health care system costs
- Lessened psychological impacts about knee “findings”
- No surgical costs
- No surgical risks
- Pain (both acute and longstanding)
- Heart disease
- Lung disease
- Diabetes
- Anxiety
- Depression
- Sleep disturbances
- Falls
- Chronic fatigue
- Memory loss
- Muscle loss
- High blood pressure
- High cholesterol
- High stress
- Low self-esteem
- And more!